Ever wonder how the ancient Romans fed their armies? What the pioneers cooked along the Oregon Trail? Who invented the potato chip...and why? So do we!!! Food history presents a fascinating buffet of popular lore and contradictory facts. Some experts say it's impossible to express this topic in exact timeline format. They are correct. Most foods are not invented; they evolve. We make food history fun.
In 2015, New Jersey librarian Lynne Olver passed away at the age of 57 after a months-long battle with a rare form of leukemia. She left behind a husband, two children, several cats, and the internet’s largest repository of chronologized food history. The cats are taken care of, but the Food Timeline needs a steward.
Who is Lynne Olver?A food historian with a masters in library science, Lynne created the Food Timeline in March 1999 and over the next 14 years welcomed 35 million readers and, at no charge to anyone, answered 25 thousand questions. She worked regularly with students, teachers, media, culinary professionals, cook book authors/editors,living history museums, and the general public worldwide providing original content, background material, fact checking services, and document delivery.
By the time she died New York health officials had identified more than 400 other healthy carriers of Salmonella typhi, but no one else was forcibly confined or victimized as an “unwanted ill”.
Zuerst waren Bürger, Politik und Wissenschaft in der Corona-Krise im Gleichklang. Das ändert sich rapide, und das ist gefährlich.Von Ranga Yogeshwar
A guide to making sense of a problem that is now too big for any one person to fully comprehend
To stay healthy, humans and some other animals rely on a complex community of bacteria in their guts. But research is starting to show that those partnerships might be more the exception than the rule.
“Every organism that exists has three and a half billion years of evolutionary history behind it, many millions or tens or hundreds of millions of which are not shared with organisms that we use as models,” Sanders said. Scientists’ emerging awareness of the diverse relationships that animals share with microbes “should make us really cautious about drawing inferences using fruit flies as models for gut microbiome importance or interactions, because fruit flies might be operating from a very different fundamental starting point compared to humans. It’s the same thing with mice.”
MIT has developed a new model of the spread of COVID-19 infection, based on publicly available data, combined with established epidemiological equations about outbreaks, and neural network-based inference. The model, described in a new report, proves accurate when trained on data spanning late January to early March in terms of anticipating the actual spread leading up to April 1 in different regions around the world, and it indicates that any immediate or near-term relaxation or reversal of quarantine measures currently in place would lead to an “exponential explosion” in the number of infections.
MIT’s model shows that the current infection plateau for COVID-19 in the U.S. and Italy will both take place sometime in the next week or so, which matches existing predictions available. That sounds like promising news, and it is in terms of the number of infected patients, and the impact on the healthcare system, but it absolutely should not be interpreted as meaning that this is when it’s okay to start relaxing the measures in place.In fact, the study concludes that by “relaxing quarantine measures too soon, we have predicted that the consequences would be far more catastrophic,” according to model developer and MIT mechanical engineering professor George Barbastathis, when compared to a similar second-wave resurgence that occurred in Singapore after it began relaxing its own measures too early.
So throughout most of the country we are going to add fuel to the viral fire by reopening. It's going to happen if I like it or not, so my goal here is to try to guide you away from situations of high risk.
The Practical Guide for Health Risk Communication, which is a collaborative effort between BMJ Publishing Group, CEDARthree, Istituto Superiore di Sanità and Zadig Srl, is a main outcome of the TELL ME project. It is a collection of four guidance documents geared towards health care professionals, public health officials, decision-makers in the fields of infectious disease management and communication.The Practical Guide for Risk Communication offers practical recommendations and tools to support the development of evidence-based messages, tailored for different sub-populations and target groups across various cultural contexts with the aim to further improve risk communication and the management of national or international public health threats at different phases of a major infectious disease outbreak.
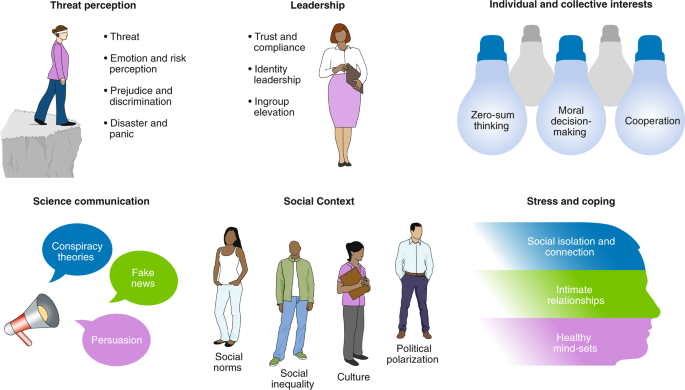
Forty-three experts highlight some key insights from the social and behavioural sciences for effective response to the COVID-19 pandemic and point out important gaps researchers should move quickly to fill in the coming weeks and months.
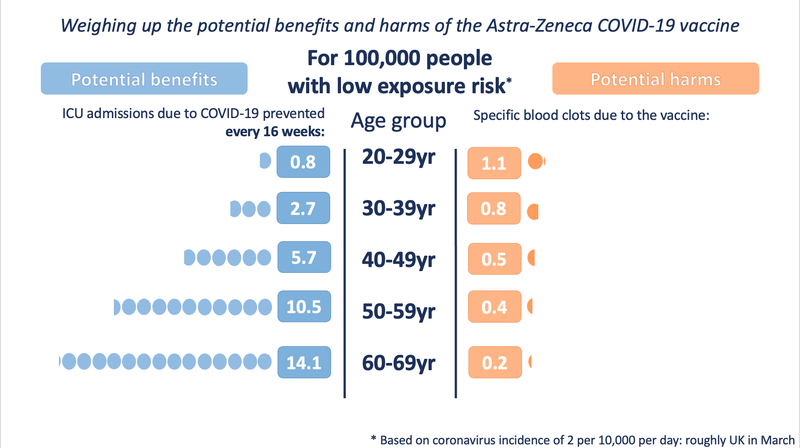
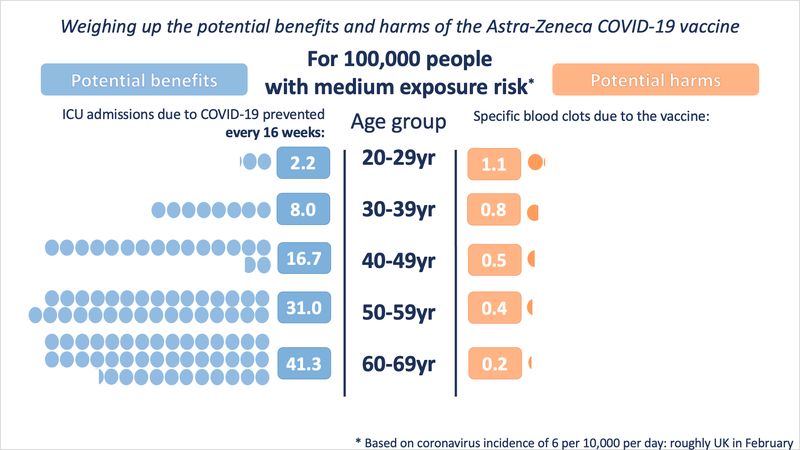
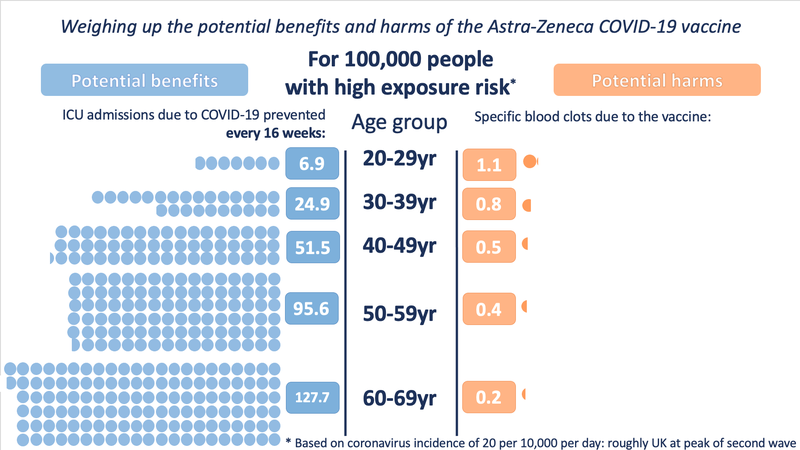
All medical treatments have potential harms as well as potential benefits, and it's important to be able to weigh these against each other. With vaccines, the benefits are particularly complex as they can involve benefits to others as well as to ourselves - and the harms can feel particularly acute because we take vaccines when we are healthy, as a preventative measure.
These fact boxes are supposed to help you weigh the benefits and harms of a vaccination against COVID-19. The information and numbers in this fact box represent no final evaluation. They are based on the best scientific evidence currently available. The fact boxes were created in a collaboration between the Robert Koch Institute (RKI, Berlin) and the Harding Center for Risk Literacy (University of Potsdam).
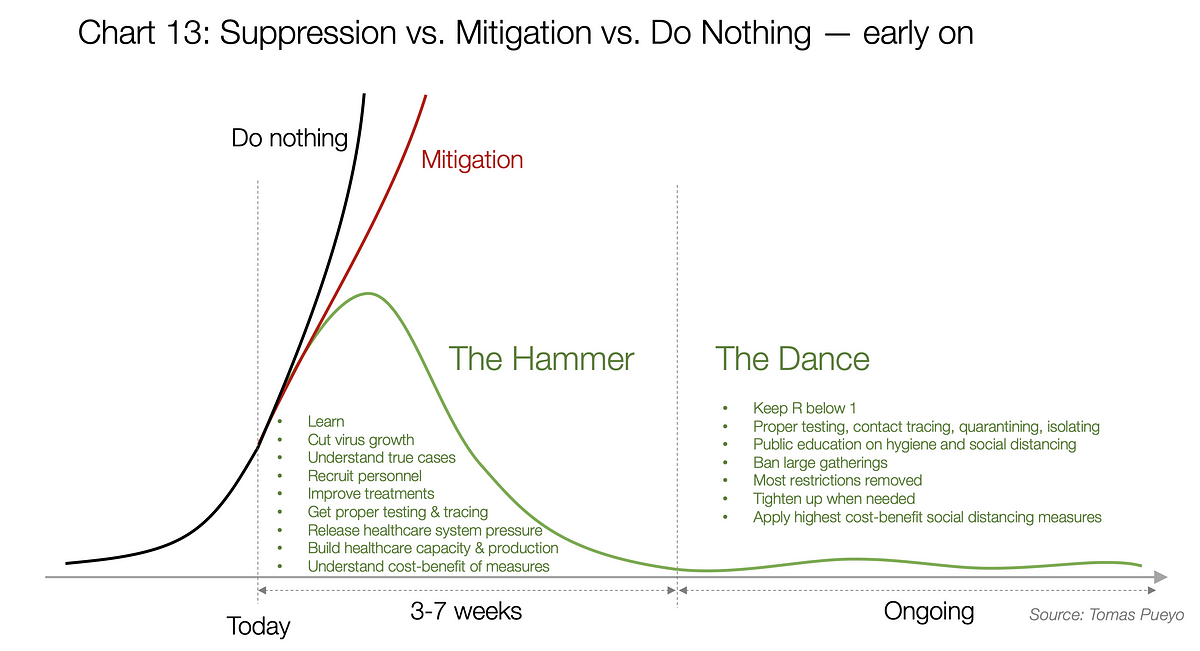
What the Next 18 Months Can Look Like, if Leaders Buy Us Time
Telling everyone to wear masks indoors has a sociological effect. Grocery stores and workplaces cannot enforce mask wearing by vaccination status. We do not have vaccine passports in the U.S., and I do not see how we could. Places can either say “wear a mask regardless” or just accept that people who don’t want to wear one will not.In the early days of the pandemic it made sense for everyone to wear a mask, not just the sick — as the C.D.C. and the World Health Organization were recommending — if only to relieve the stigma of illness. Now, as we head toward the endgame, we need to apply the same logic but in reverse: If the unvaccinated still need to wear masks indoors, everyone else needs to do so as well, until prevalence of the virus is more greatly reduced.Even if the only people not protected by the vaccines were those hesitant to use them or who had false beliefs about them, public health principles would not allow us to say that any threat to their health is their problem, at least not while the virus is still spreading at substantive levels. Infectious diseases create risks for others.There are those who are not yet vaccinated because they haven’t managed to navigate the process, or have started late, or are concerned because of bad experiences with the medical establishment. The immunocompromised remain vulnerable. Even if the unvaccinated were all conspiracy theorists and dead-end anti-vaxxers, we would need to take virus levels into account before discounting the risks even to them.Plus, Covid-19 can still terribly burden our health resources, especially in those areas that still have many unvaccinated adults.The C.D.C. guidelines are essentially implying that the risk that the vaccinated will transmit the virus to others, including their unvaccinated children, is so vanishingly low that it is not worth worrying about. But if that’s their position, they should state it clearly and explain it, not just say that “fully vaccinated people have a reduced risk of transmitting” the virus.And is the expectation that the unvaccinated will all simply go with the guidance and stay masked? That does not fit with what we’ve observed in this country over the past year, especially with the ongoing polarization over these questions.
AbstractSweden was well equipped to prevent the pandemic of COVID-19 from becoming serious. Over 280 years of collaboration between political bodies, authorities, and the scientific community had yielded many successes in preventive medicine. Sweden’s population is literate and has a high level of trust in authorities and those in power. During 2020, however, Sweden had ten times higher COVID-19 death rates compared with neighbouring Norway. In this report, we try to understand why, using a narrative approach to evaluate the Swedish COVID-19 policy and the role of scientific evidence and integrity. We argue that that scientific methodology was not followed by the major figures in the acting authorities—or the responsible politicians—with alternative narratives being considered as valid, resulting in arbitrary policy decisions. In 2014, the Public Health Agency merged with the Institute for Infectious Disease Control; the first decision by its new head (Johan Carlson) was to dismiss and move the authority’s six professors to Karolinska Institute. With this setup, the authority lacked expertise and could disregard scientific facts. The Swedish pandemic strategy seemed targeted towards “natural” herd-immunity and avoiding a societal shutdown. The Public Health Agency labelled advice from national scientists and international authorities as extreme positions, resulting in media and political bodies to accept their own policy instead. The Swedish people were kept in ignorance of basic facts such as the airborne SARS-CoV-2 transmission, that asymptomatic individuals can be contagious and that face masks protect both the carrier and others. Mandatory legislation was seldom used; recommendations relying upon personal responsibility and without any sanctions were the norm. Many elderly people were administered morphine instead of oxygen despite available supplies, effectively ending their lives. If Sweden wants to do better in future pandemics, the scientific method must be re-established, not least within the Public Health Agency. It would likely make a large difference if a separate, independent Institute for Infectious Disease Control is recreated. We recommend Sweden begins a self-critical process about its political culture and the lack of accountability of decision-makers to avoid future failures, as occurred with the COVID-19 pandemic.